Introduction
Airway management is a critical skill in clinical practice, especially for patients with tracheostomy tubes. This guide outlines the procedure for addressing tracheostomy cuff failure, detailing the steps required to ensure patient safety, airway security, and successful tube exchange.
Initial Assessment
The first sign of a problem in this scenario was a notification from the anesthesia team regarding a significant air leak. Visual inspection of the oral cavity revealed air bubbles and a gurgling sound, strongly indicating that air was escaping from the trachea. Possible causes include:
- The endotracheal tube cuff is deflated and needs additional air to prevent leakage.
- The endotracheal tube has become dislodged, with the cuff now above the true vocal cords (risking extubation).
- The endotracheal tube cuff is ruptured, allowing air to escape around it.
Among these, the most critical concern is to rule out the displacement of the endotracheal tube above the level of the true vocal cords.
Verification of Tube Placement
To confirm the appropriate placement of the endotracheal tube (ETT), use a laryngoscope for direct visualization of the tube’s position. It is essential that the tube is positioned below the vocal cords. Additionally, confirming the return of carbon dioxide (CO2) in the ventilation circuit provides further assurance that the tube is correctly placed within the airway.
Despite these confirmations, the persistent air leak requires further intervention. If re-inflating the cuff fails to maintain cuff pressure, this indicates a ruptured cuff, necessitating a ETT replacement.
Preparing for Tube Exchange
Once it’s determined that a new tube is required, preparation is key. Start by notifying the anesthesiologist and increase the patient’s pulmonary reserve by temporarily administering high-flow oxygen.
Gather and organize all necessary equipment:
- A heavy bougie to guide the new tube into position.
- A laryngoscope (Anterior commissure, etc) of your choice. A GlideScope (Laryngoscope with video monitor) might also be useful.
- A flexible bronchoscope for visual confirmation or fiberoptic intubation if necessary.
- A tracheostomy tray in case an emergent tracheostomy is required.
Executing the Tube Exchange
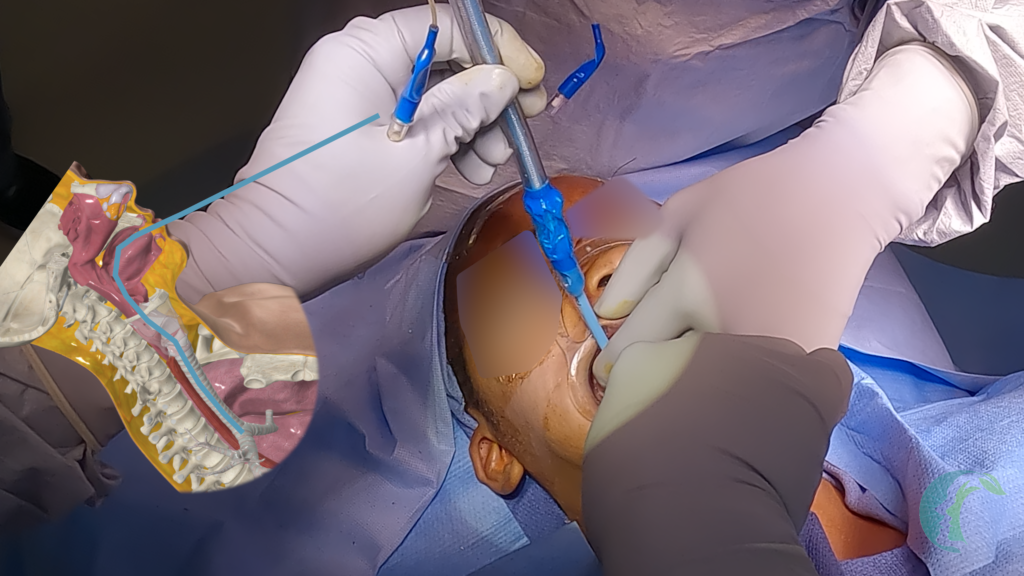
- Insert the Bougie: Begin the tube exchange by threading the bougie through the old endotracheal tube. Ensure it is placed deep into the trachea, ideally at the level of the carina, before removing the old tube.

- Remove the Old Tube: Carefully remove the old endotracheal tube while keeping the bougie in place. The bougie provides guidance for the new tube during the exchange.
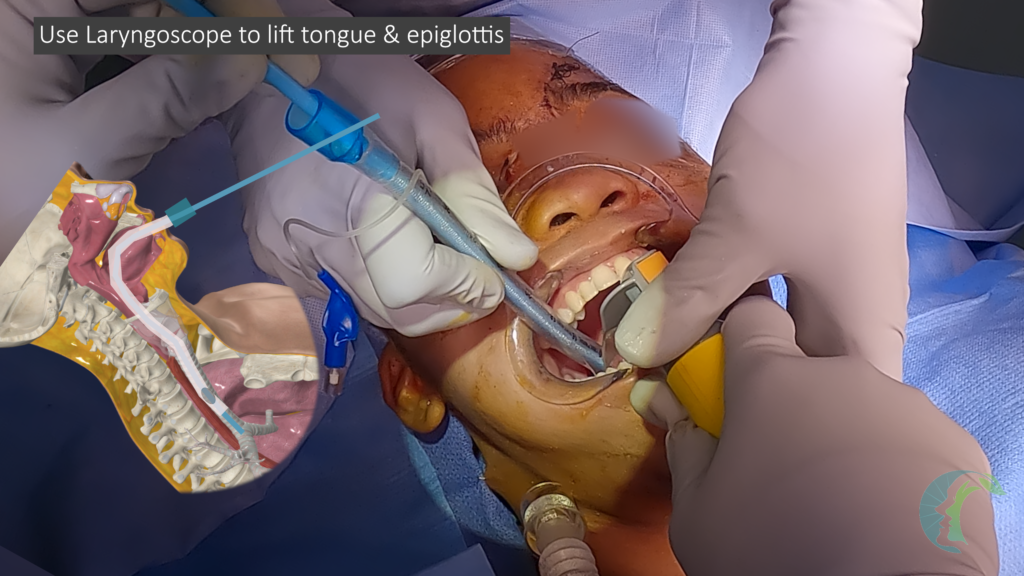
- Place the New Tube: Insert the new endotracheal tube over the bougie, ensuring not to apply excessive pressure. If soft tissue obstruction related resistance is encountered, use a gentle corkscrew motion to maneuver the tube. In cases of tongue or floor-of-mouth edema, perform a jaw thrust or use a laryngoscope to lift the tongue for better access (this is not always necessary but helpful if meeting a lot of resistance from tongue or epiglottis).
- Confirm Placement: Once the new endotracheal tube is in place, remove the bougie. Inflate the cuff and connect the tube to the ventilator circuit. Confirm proper placement by checking end-tidal CO2 with the anesthesiologist.
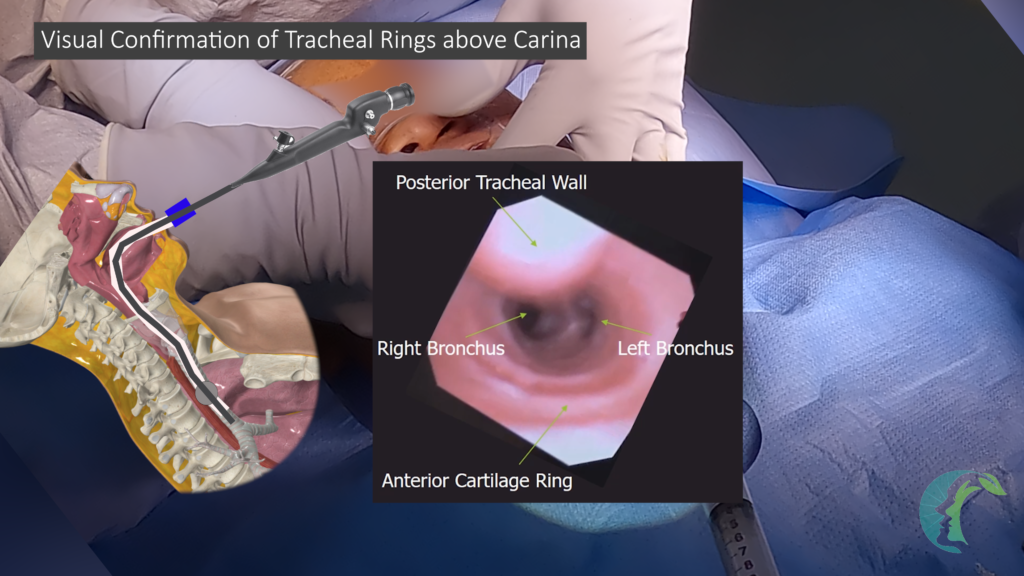
- Address Concerns: If there is any concern about improper placement, use a laryngoscope to confirm proper placement. You can also consider using a flexible bronchoscope to visualize tracheal rings and confirm that the tube is within the trachea. After confirming end-tidal CO2, check that the tube is not too deep—position it proximal to the carina to ensure effective ventilation. Bilateral breath sounds and bronchoscope visualization of the carina can further verify correct placement.
- Re-establish Airway if Necessary: If the tube is incorrectly placed in the esophagus, remove it and re-establish the airway with a properly placed endotracheal tube.
- Secure the Tube: Once the tube is correctly positioned, secure it to prevent displacement.
Conclusion
Managing a malfunctioning tracheostomy tube requires prompt and effective action. By following these steps—initial assessment, tube placement verification, preparation, exchange execution, and final confirmation—you can ensure successful airway management. Continuous monitoring and the ability to adapt to challenges are crucial for optimal patient outcomes.