By Kathryn Wie MD, Thomas S. Lee MD, FACS
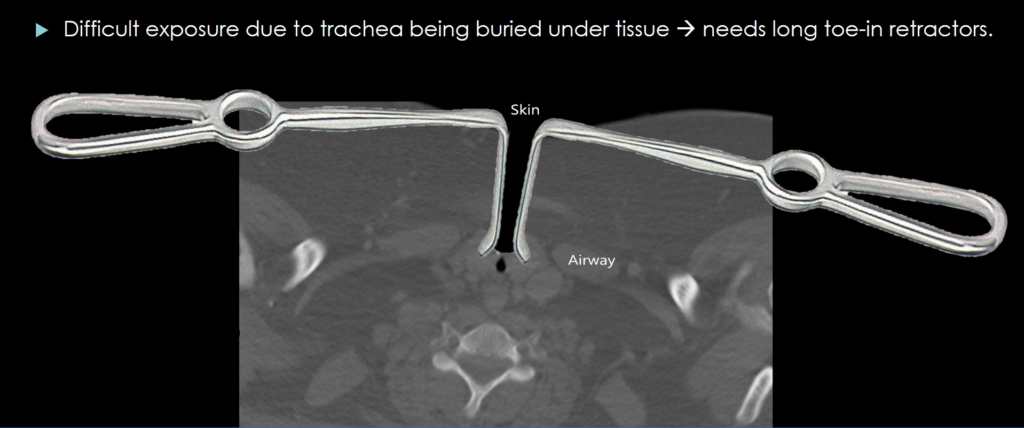
This lecture describes a surgical case report of an obese neck adult patient needing urgent tracheostomy due to severe proximal tracheal stenosis.
Discusses technique that can be employed when trach obturator is unsuccessful in fresh trach placement from anterior tracheal wall collapse.
At the conclusion of this lecture, the learner should be able to:
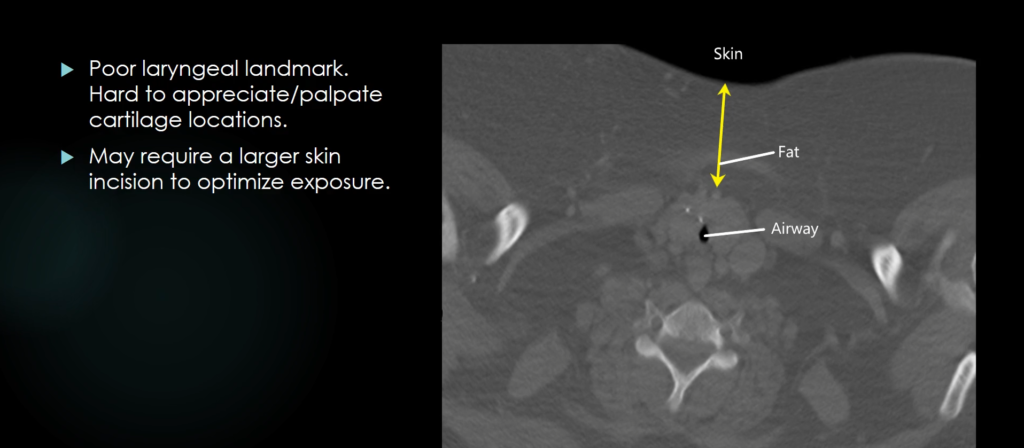
Unique Obese Neck Anatomy that makes Trach Placement Challenging:
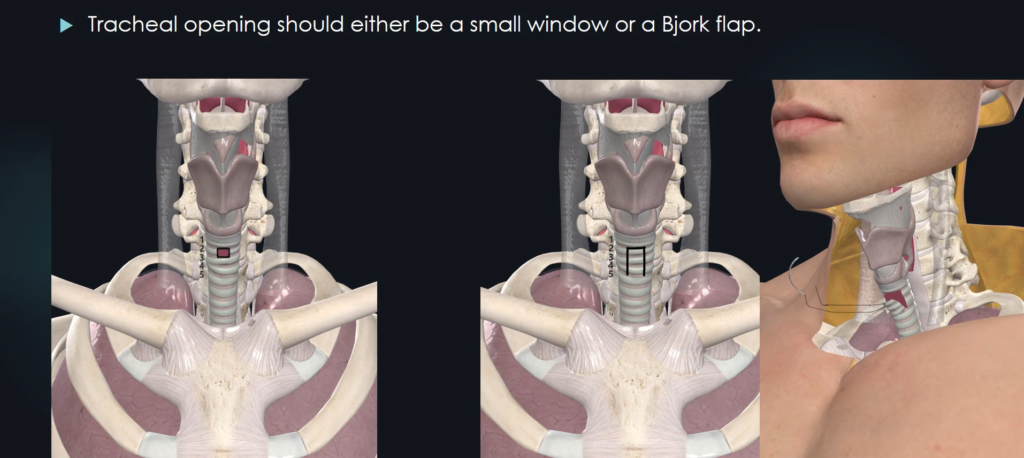
Preferred Tracheal Opening Techniques in Obese Necks?
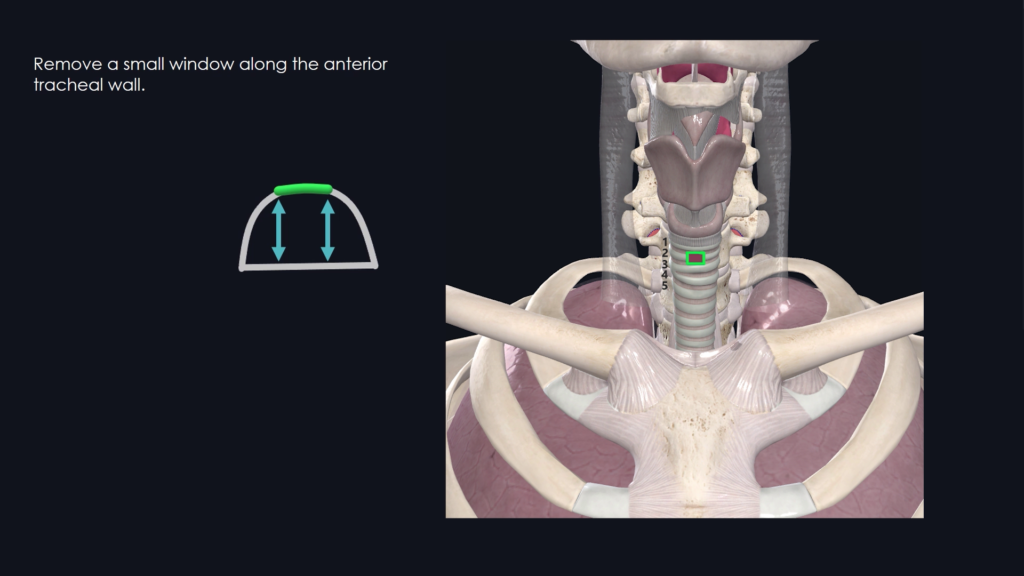
Small anterior tracheal window (while preserving tracheal height) or Bjork Flap.
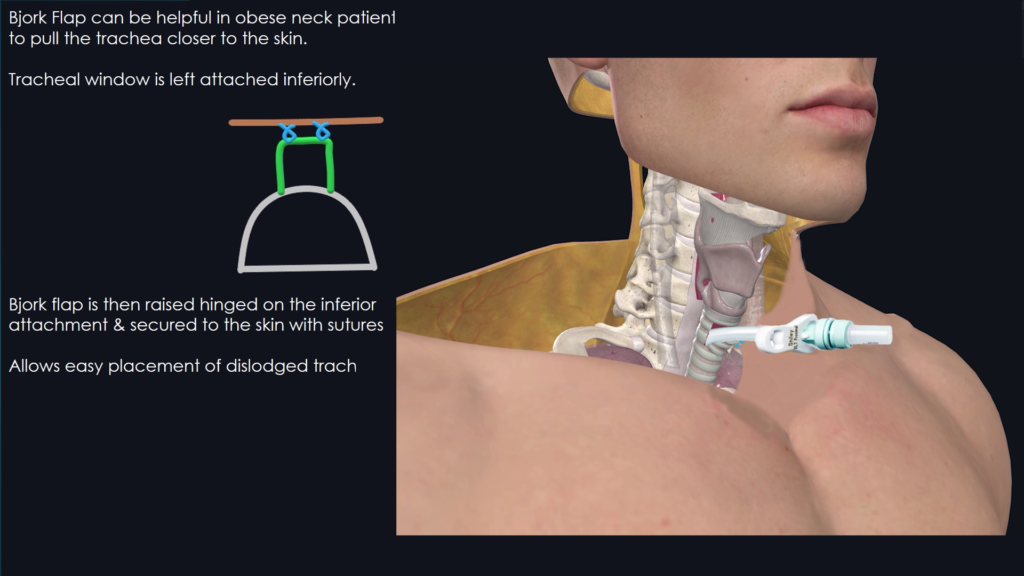
Aside from the Bjork flap technique, another option to bring the trachea more superficial is to place temporary stay sutures.
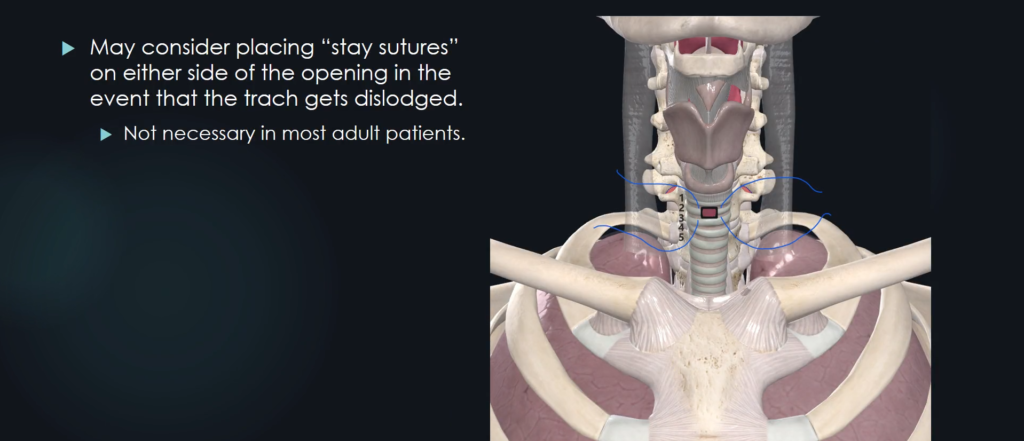
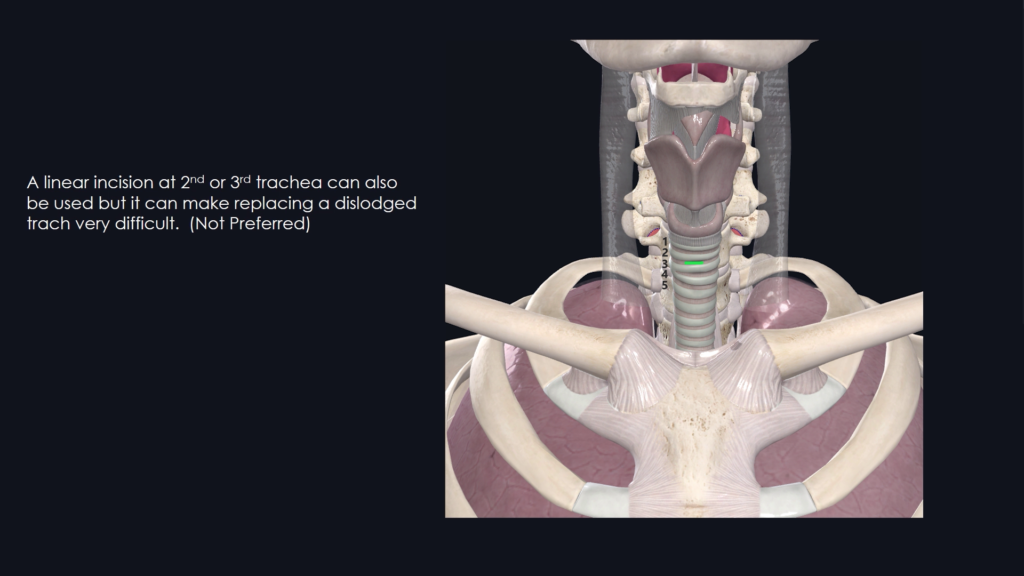
For obese neck patient’s trach opening, avoid making a linear incision between tracheal rings as the tracheal rings can collapse back on itself.
It can make trach replacement very difficult once the trach gets dislodged.
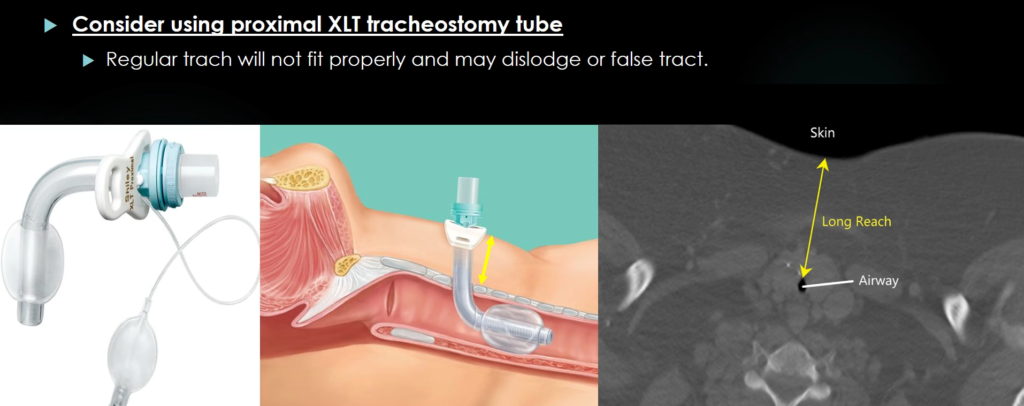
What is the difference between Proximal XLT & Distal XLT tracheostomy tubes?
Which one to use in obese neck patients?
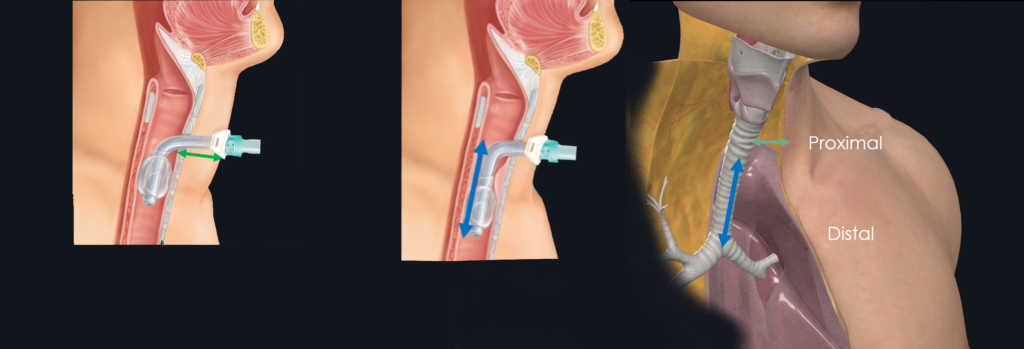
–Proximal XLT trach = Use for obese/large neck patient with large neck skin/soft tissue present anterior to the trachea
-Distal XLT Trach = Use for tracheal stenosis that exists distal to the tracheal opening. ex. tracheomalacia, tracheal collapse, tracheal mass
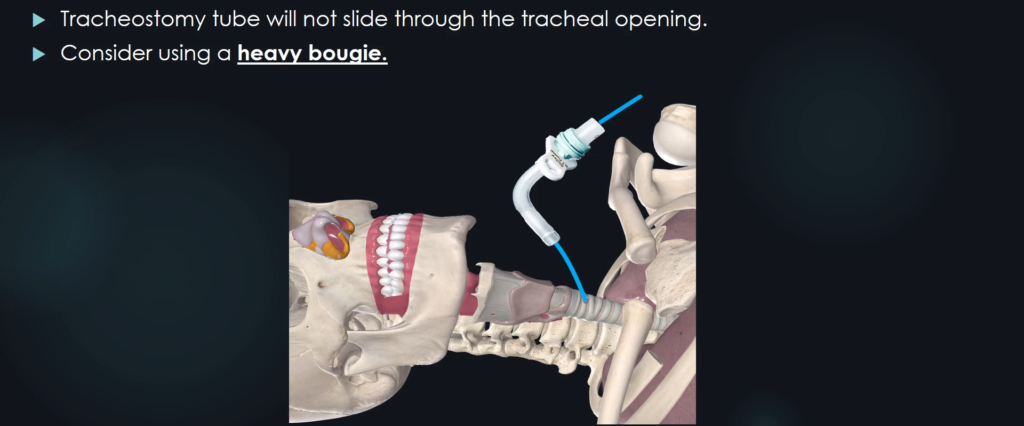
What to do if an obturator is not effective in placing a new tracheostomy tube into the airway?
Using an obturator will be effective in trach placement in vast majority of the time. But in that rare situation when it is not working, try using a heavy bougie to thread it into the airway.
Surgical Case Report
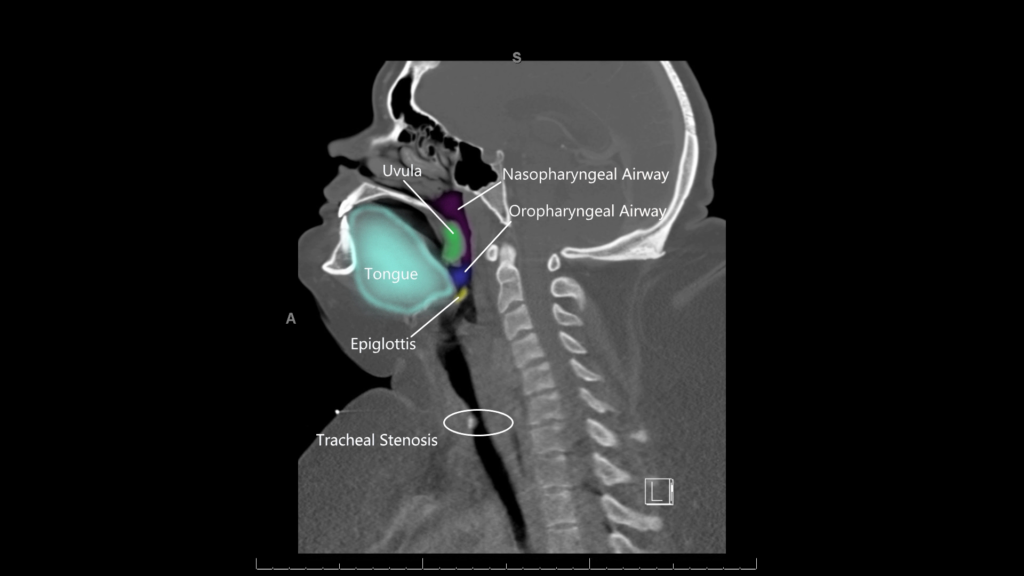
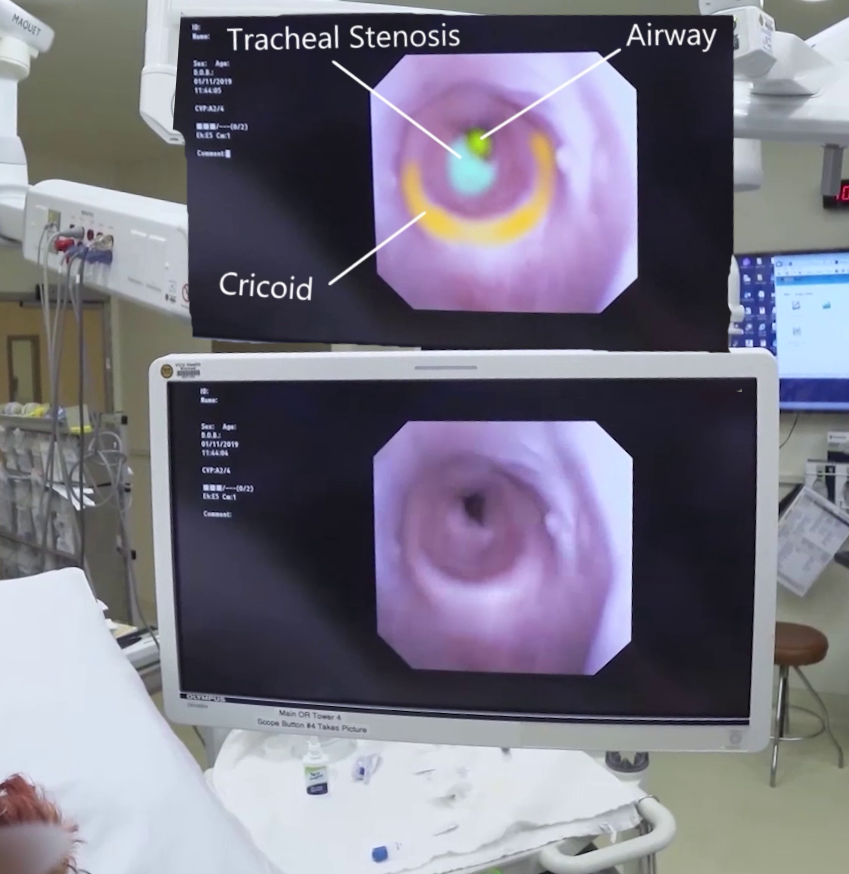
Obese female with previous history of tracheostomy that was decannulated presenting with hypercarbic respiratory failure needing urgent tracheostomy placement. Patient was noted to have proximal tracheal stenosis at the site of previous trach placement from loss of support along the anterior tracheal cartilage. In the operating room, the patient underwent flexible, transnasal intubation and underwent tracheostomy placement. The case was remarkable due to the difficulty in tracheostomy placement from collapsing anterior tracheal wall that is located in a deep surgical field. Initial attempt at trach placement with an obturator failed. A heavy bougie was used successfully to place the tracheostomy tube.
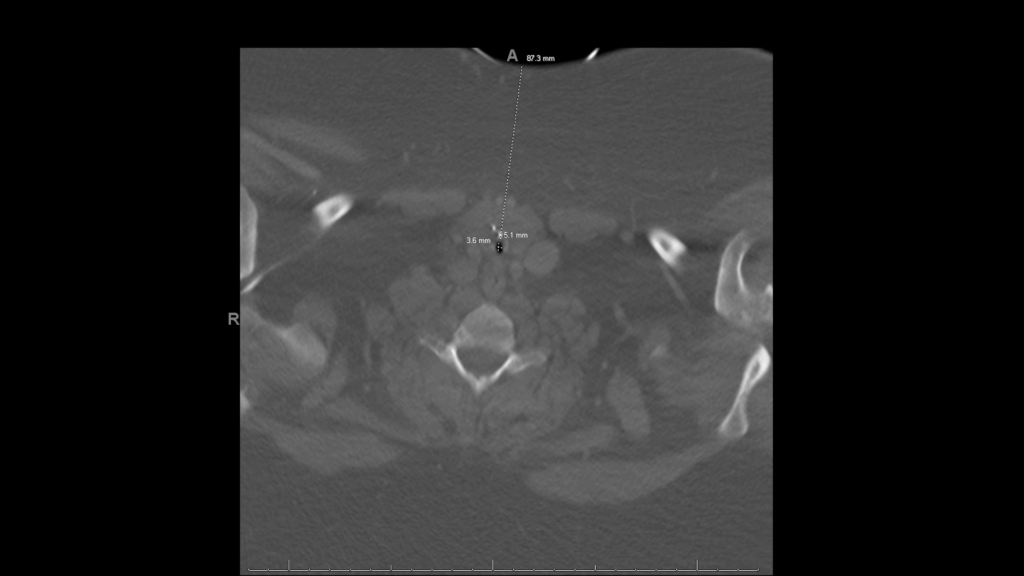
Axial CT 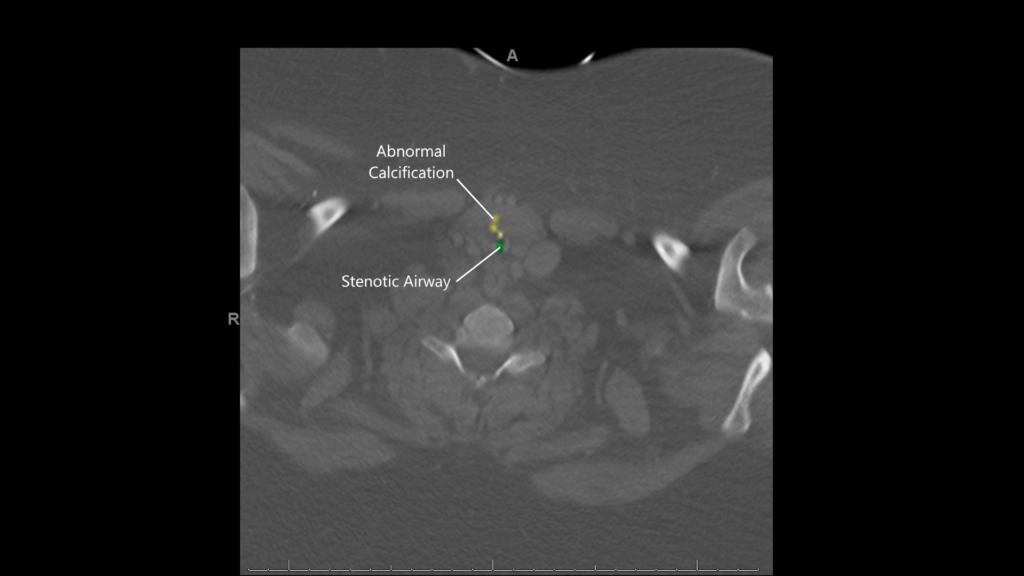
Coronal CT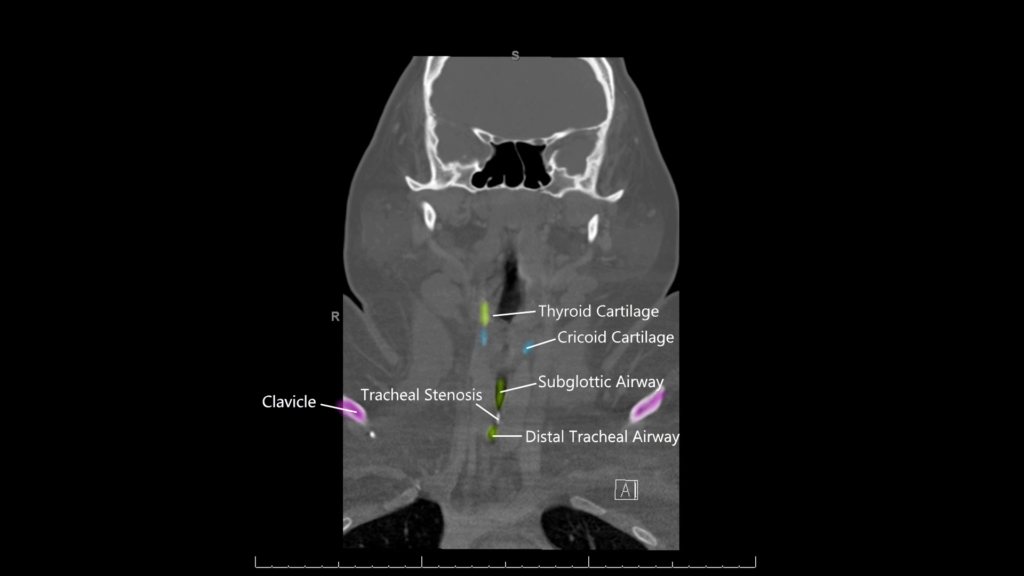
Sagittal CT